diagnostic case reports
In research applications we offer a detailed report on ICP pressure variations via surrogate ICP waveform morphology that can better support diagnostics
hydrocephalus
Application and context
Hydrocephalus is a disease caused by the abnormal accumulation of cerebrospinal fluid in the brain in one or more ventricular sinuses, causing changes in brain compliance and clinical manifestations such as headaches (intensified when the person is lying down and improved when sitting or standing), mental confusion, and losses of memory and balance. It can affect adults and children and differential diagnosis is often difficult and time-consuming, as imaging tests may be non-specific.
In adults, hydrocephalus may occur due to other diseases, such as strokes, brain tumors, trauma, and intracranial hemorrhages. In children, growth entails the need for periodic surgeries to replace ventriculoperitoneal shunts.
How brain4care may contribute to the diagnosis of hydrocephalus
- Monitoring can be performed in minutes, anywhere, without pain nor incurring in unnecessary risks to the patient
- Ability to assess changes in brain compliance related to early stages of hydrocephalus and in cases where imaging tests are non-specific
- Increases safety in prescribing invasive procedures, pointing out when they are actually needed
- Reduces the repetition of invasive procedures and exposure to radioactive agents in the diagnostic survey
Case 1 – hydrocephalus in an adult
Adult, female, 65 years old, with diagnosis of SAH (Subarachnoid Hemorrhage), Fisher III classification. Aware, responding to stimuli, oriented in time and space, undergoing intense headache at the base of the skull, with worsening in decubitus inferior at 30°.
The monitoring of NIICP (non-invasive intracranial pressure) was requested by the physician to assist in the diagnosis of hydrocephalus and intracranial hypertension.
Two monitoring sessions were performed on 12/12/18 and 12/13/18, both with changes in the decubitus position: the first 5 minutes in the horizontal dorsal decubitus position and then 5 minutes in the elevated decubitus position at 45°.
findings and medical procedure
first monitoring
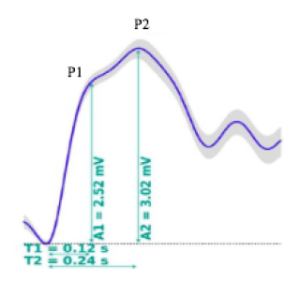
Horizontal dorsal decubitus. Change of surrogate ICP waveform (P2/P1 ratio = 1,210)
first monitoring
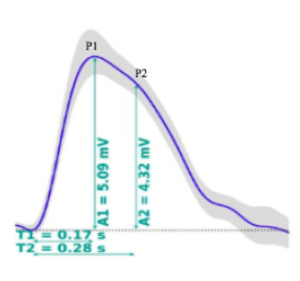
Elevated dorsal decubitus at 45°. Change of surrogate ICP waveform, but with an improvement in the P2/P1 ratio (P2/P1 ratio = 0.849)
medical procedure
Performance of lumbar puncture for CSF drainage
second monitoring
After lumbar puncture, the patient presents improved symptoms (headache). Horizontal dorsal decubitus. Surrogate ICP waveform change, but with an improvement in the P2/P1 ratio (P2/P1 ratio = 1.030)

second monitoring
Elevated dorsal decubitus at 45°. Surrogate ICP waveform change maintained, but P2> P1 ratio improved in relation to the dorsal decubitus position
horizontal (P2/P1 ratio = 0.965)
medical procedure
Due to the significant improvement in the clinical symptoms, it was decided to wait another 24 hours for reevaluation and for the discharge from the semi-intensive care unit
outcome
Patient with clinical improvement and rapid diagnosis
Case 2 – pediatric hydrocephalus
Girl, age 8, born prematurely at 32 weeks, GI, Apgar 4/8, with previous diagnoses of: grade III intracranial hemorrhage in the left ventricle and grade II in the right ventricle at 18 days of life, third ventriculostomy at the 28th day of life, placement of ventriculoperitoneal shunt (VPS) without gauging in the right ventricle at 60 days of life and change of this shunt at age 3 for a gauged valve.
New change of VPS at age 4 by a programmable siphon model, gauged at 16mmHg.
Entered the emergency room with severe headache; an eye fundus evaluation was performed and the results were normal.
Non-invasive intracranial pressure monitoring was requested for diagnostic assistance.
findings and medical procedure
first monitoring
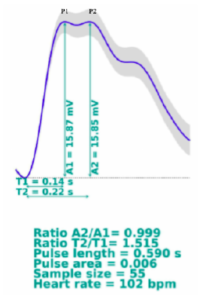
Change in brain compliance with P2> P1 (P2/P1 ratio = 0.999)
medical procedure
A new imaging examination (MRI) was performed and showed hydrocephalus, and another ventriculoperitoneal shunt (VPS) was placed in the left ventricle
first monitoring
Performed in the postoperative period after the placement of the ventriculoperitoneal shunt (VPS).
No changes in brain compliance with P1> P2 (P2/P1 ratio = 0.586)

medical procedure
Clinical evaluation with improvement of signs and symptoms, opting for hospital discharge and outpatient follow-up.
outcome
Rapid and effective diagnosis, with economy of resources and gain of quality of life for the patient and her relatives.
verification of vps valve proper function
Application and context
People with hydrocephalus have an abnormal accumulation of cerebrospinal fluid in one or more ventricular sinuses, causing a change in brain compliance. The treatment of these patients includes the surgical implantation of a valve that drains excess fluid and maintains the central nervous system in equilibrium (VPS valve). Even with the valve implanted, these patients may present clinical manifestations such as headaches, mental confusion, as well as loss of memory and balance. Determining whether or not the cause of the manifestations is related to the inadequate functioning of the valves can be difficult, especially when the results of the imaging tests do not correspond to the patients’ clinical picture.
how brain4care helps in verifying the operation of vps valves
brain4care’s non-invasive monitoring method may support the interpretation of whether there is a change in brain compliance in real time and dynamically. When comparing changes in the patient’s condition, after performing readings in the sitting and lying positions, it may be possible to identify whether the symptoms are related to the inadequate flow or to a malfunction of the valve, assisting in the definition of the diagnosis.
- If the patient’s symptoms worsen when they are lying down, and the ICP curve is altered in this position, this is a sign that the valve is not providing the necessary flow
- If the symptoms worsen when the patient is seated and the ICP curve changes in this position, this is a sign that the valve is draining more than necessary
potential benefits and impacts
- Monitoring can be performed in minutes, in various care settings, without causing pain or entailing risks to the patient
- It allows for a quick and accurate determination of the actual operation of the VPS valve, contributing to accelerate and qualify the definition of the diagnosis
- This provides a new perspective of analysis for the diagnosis, especially compared to non-specific imaging tests
- It also reduces the repetition of invasive procedures and exposure to radioactive agents in the diagnostic survey
related scientific article
Evaluation of a non-invasive method for monitoring intracranial pressure in children and adolescents with hydrocephaly – Master’s Thesis
Matheus Fernando Manzolli Ballestero
clinical case 1 – intracranial hypertension caused by infections of the central nervous system (cns)
Girl, age 11, complaining of headaches and worsening of visual acuity. At physical examination, ECG 15, non-photoreceptor pupil D, pupil E photoreagent, presence of nuchal rigidity, without motor or sensory deficits. A neurosurgery evaluation was requested due to suspicion of intracranial hypertension and central venous thrombosis. Head MRI, eye fundus examination, cerebrospinal fluid collection with spinal anesthesia, non-invasive monitoring of intracranial pressure and laboratory tests were requested. Inpatient care was chosen due to the necessity of follow-up with pediatric specialties that are not available in the original service.
findings and medical procedure
first monitoring
After the head CT scan, there was a change in surrogate ICP waveform with P2> P1 (P2/P1 ratio = 1.124).

medical procedure
Performing a CSF puncture, with opening pressure of 40 cmH2O and closing pressure 29 cmH2O.
Introduction of acetazolamide and lumbar punctures for control and relief of intracranial hypertension.
second monitoring
On the seventh day of hospitalization, improvement of surrogate ICP waveform with P1>P2 (P2/P1 ratio = 0.856), which may indicate the efficacy of the drug therapy and invasive lumbar puncture therapy.

medical procedure
Performance of a new lumbar puncture, presenting opening pressure of 9 cmH2O (within the normality standards), suspending the use of acetazolamide.
third monitoring
Performed on the 16th day of inpatient care. Surrogate ICP waveform within normal range with P1>P2 (P2/P1 ratio = 0.703), important clinical improvement with absence of headache and nuchal stiffness, but maintaining a significant decrease in visual acuity, especially in the left eye.

medical procedure
Hospital discharge with outpatient case follow-up
outcome
Differential diagnostic assistance in cases of difficult management with negligible financial impact compared to gain in time and quality of life associated with the reversion of infection.
intracranial hypertension caused by central nervous system (cns) infections
Application and context
Intracranial hypertension (ICH) is a clinical condition characterized by increased pressure inside the skull, compressing all structures of the brain, causing, among other things, permanent loss of vision and even death.
One of the possible causes of ICH is a CNS infection. They are very serious, caused by neglect in treating infectious diseases of other parts of the body, loss of immune response and infections related to health care (iatrogenesis).
The diagnosis of CNS infection is simple, but the identification of ICH requires invasive procedures (lumbar puncture).
how brain4care contributes to diagnose CNS infections
brain4care’s non-invasive monitoring allows simple, fast, safe and painless access to changes in brain compliance via monitoring and interpretation of surrogate ICP waveform and associated parameters at all moments of the patient’s journey, accelerating and expanding access to the diagnosis of CNS infections.
By pointing out changes in brain compliance in real time, the method helps in defining the diagnosis and monitoring the response to medication.
potential benefits and impacts
- Monitoring can be performed in minutes, in various care settings, without causing pain or entailing risks to the patient
- It allows to accelerate the definition of the diagnosis, improving decision making and patient follow-up
- It contributes to reducing the risk of irreversible sequelae such as loss of vision and reduces the patient’s risk of death
- It also reduces the unnecessary repetition of invasive procedures and exposure to radioactive agents in the diagnostic survey
related scientific article
Noninvasive intracranial pressure monitoring for HIV-associated cryptococcal meningitis.
Braz J Med Biol Res. 2017
Bollela VR, Frigieri G, Vilar FC, Spavieri DL Jr, Tallarico FJ, Tallarico GM, Andrade RAP, de Haes TM, Takayanagui OM, Catai AM, Mascarenhas S.
clinical case 1 – intracranial hypertension caused by infections of the central nervous system (cns)
Girl, age 11, complaining of headaches and worsening of visual acuity. At physical examination, ECG 15, non-photoreceptor pupil D, pupil E photoreagent, presence of nuchal rigidity, without motor or sensory deficits. A neurosurgery evaluation was requested due to suspicion of intracranial hypertension and central venous thrombosis. MRI of skull, eye fundus examination, spinal fluid collection with spinal anesthesia, non-invasive monitoring of intracranial pressure and laboratory tests were requested. Inpatient care was chosen due to the necessity of follow-up with pediatric specialties that are not available in the original service.
findings and medical procedure
first monitoring
After the CT scan of the skull, there was a change in surrogate ICP waveform with P2>P1 (P2/P1 ratio = 1.124).

medical procedure
Performing a CSF puncture, with opening pressure of 40 cmH2O and closing pressure 29 cmH2O.
Introduction of acetazolamide and lumbar punctures for control and relief of intracranial hypertension.
second monitoring
On the seventh day of hospitalization, improvement of surrogate ICP waveform with P1>P2 (P2/P1 ratio = 0.856), which may indicate the efficacy of the drug therapy and invasive lumbar puncture therapy.

medical conduct
Performance of a new lumbar puncture, presenting opening pressure of 9 cmH2O (within the normality standards), suspending the use of acetazolamide.
third monitoring
Performed on the 16th day of inpatient care. Surrogate ICP waveform within the normal range with P1>P2 (P2/P1 ratio = 0.703), important clinical improvement with absence of headache and nuchal stiffness, but maintaining a significant decrease in visual acuity, especially in the left eye.

medical procedure
Hospital discharge with outpatient case follow-up.
outcome
Differential diagnostic assistance in cases of difficult management with negligible financial impact compared to gain in time and quality of life associated with the reversion of infection.